

This SLO describes the EM clinician as someone who understands patient safety and can effectively advocate for it as a consultant in the ED.
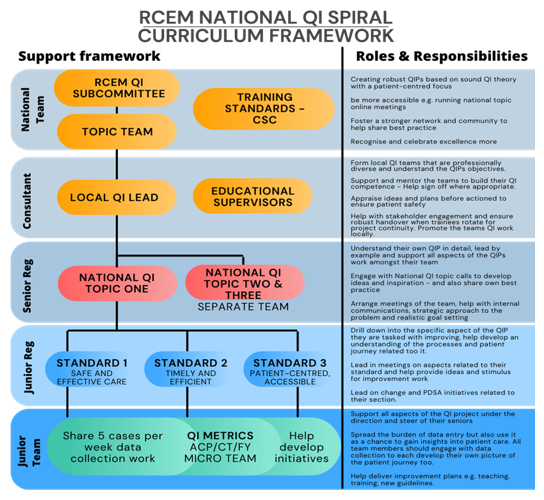
In developing the Key Capabilities there is a requirement to be able to identify areas that need changing in the ED, to design improvements and to be able to implement them. This requires knowledge of techniques, theoretical underpinnings and their practical application. It also requires the leadership skills to work effectively with others, to be tenacious, imaginative and at times bold.
This is the QI journey – see below.

Development against these requirements requires feedback and reflection. Built into the Programme of Learning and Assessment throughout are the key leadership, interpersonal and human elements of being effective in this SLO.
Domain 1: Professional values and behaviours
Domain 2: Professional skills
- practical skills
- communication and interpersonal skills
- dealing with complexity and uncertainty
- clinical skills (history taking, diagnosis and medical management; consent; humane interventions; prescribing medicines safely; using medical devices safely; infection control and communicable disease)
Domain 3: Professional knowledge
- professional requirements
- national legislative requirements
- the health service and healthcare systems in the four countries
Domain 4: Capabilities in health promotion and illness prevention
Domain 5: Capabilities in leadership and teamworking
Domain 6: Capabilities in patient safety and quality improvement
- patient safety
- quality improvement
For the full list of key capabilities and descriptors, please refer to the RCEM 2021 curriculum (2025 update)
Key ACCS capabilities
At completion of ACCS a trainee will:
- be able to contribute effectively to a departmental quality improvement project
Key EM capabilities
At completion of Intermediate training a trainee will:
- be able to describe their involvement and show an understanding of QI methods and reflect on a Quality Improvement Project they have been involved in
At completion of Higher training a trainee will:
- be able to provide clinical leadership on effective Quality Improvement work
- be able to support and develop a culture of departmental safety and good clinical governance
Intermediate & Higher Descriptors
- Makes patient safety a priority in clinical practice
- Raises and escalates concerns where there is an issue with patient safety or quality of care
- Demonstrates commitment to learning from patient safety investigations and complaints
- Shares good practice appropriately
- Contributes to and delivers quality improvement
- Understands basic Human Factors principles and practice at individual, team, organisational and system levels
- Understands the importance of non-technical skills and crisis resource management
- Recognises and works within limit of personal competence
- Avoids organising unnecessary investigations or prescribing poorly evidenced treatments
QI is embedded within the Programme of Learning at all stages of training, and the requirements of the curriculum reflect growing expertise and responsibility in this subject over time. The expectation is that trainees can evidence learning of the entire QI journey by the end of their training.
Trainees have access to a multitude of resources to help them develop in QI. Education programmes are available locally, regionally, nationally and on-line. Details and links can be found in the Resources section of this SLO as well as being signposted on the RCEM website. Local QI leads will also be able identify other opportunities. Most Emergency Departments will have ongoing improvement activity. Participation in the national RCEM QI programme will also be beneficial for development – see below.
Evidence of engagement in any/all of these activities can be used to demonstrate the requirements of SLO 11 at ARCP. Note that the Academy of Medical Royal Colleges in ARCP guidance states that “trainees do not need to design, lead, and project manage entire QI projects to satisfy curriculum requirements”.
The Assessment Schedule for the RCEM curriculum has been developed to best meet its aims and objectives. Two of the educational principles that have been considered in developing EM capabilities have been ‘spacing’ and ‘Interleaving’. These terms mean that there is likely to be better retention of knowledge and integration if curricular elements are introduced early, returned to for reinforcement, and if the layering of greater complexity is interspersed with other curricular content.
The GMC require all curricula to include the ability to undertake quality improvement activity in all stages of training as part of their Generic Professional Capabilities. The development and application of the underpinning knowledge and skills starts in ACCS and builds throughout training to completion.
Quality improvement capabilities are within the Programme of Learning at all stages of training, and the requirements of the curriculum reflect growing expertise and responsibility in this subject over time. The expectation is that trainees can evidence learning of the entire QI journey by the end of their training.
How is this SLO assessed?
Assessment in the workplace
Trainees at all stages are expected to demonstrate some activity in this SLO in each year of training. It is recognised that the extent of this may vary to a degree year-by-year according to trainees’ activity against the other generic SLOs. By the end of training trainees are required to provide sufficient evidence to at least a satisfactory standard for both HST Key Capabilities.
All activity relating to quality improvement is relevant and the list of evidence that might be used is not reductive in any way. Some trainees may be inspired by the topic and seek to stretch further in this area. The key capabilities that frame what is required at each stage of training and it is important to note that these capabilities can be acquired in numerous ways as described in the programme of learning and RCEM website.
EM Quality Improvement Assessment Tool (EM QIAT)
The EM QIAT form, found on the ePortfolio, is to be used by trainees in each year of training and completed in time for review by their educational supervisor in preparation for ARCP. The form captures all QI-related activity during the training year and maps it to the QI journey. It also includes the trainee’s own reflections as well as their supervisor’s feedback.
A breadth of experience can be recorded and reflected upon when using the QIAT which will support the trainee in considering their own strengths and weaknesses in relation to QI activity. Examples include involvement in a project team; leading a project team or a section within a larger project; QI learning; coaching a QI team; contributing to running the department QI programme.
Trainees can include any QI activity they have found valuable, both inside and outside the ED, whether it is directly patient-focused, or focusing on education & training, staff wellbeing or environmental sustainability.
There is an expectation that each year builds on the previous to show growth such that by the time of completion of EM training the trainee will be able to demonstrate coverage of the entire journey.
Note that the Academy of Medical Royal Colleges in ARCP guidance states that “trainees do not need to design, lead, and project manage entire QI projects to satisfy curriculum requirements”
Educational review
Summative assessment each year is a judgement by the Educational Supervisor and recorded on the ACCS ESR form, with subsequent overview from the ARCP panel. By the end of the two years of ACCS training, trainees are required to provide sufficient evidence to at least a satisfactory standard for the key capability of this SLO.
Review of the EM-QIAT
The Educational Supervisor gives a final rating following review of the EM-QIAT. This is reviewed along with all other SLOs at ARCP. Review of the EM-QIAT by the Educational Supervisors can be supported by appropriately trained departmental QI leads or other local equivalents.
Note that the Academy of Medical Royal Colleges in ARCP guidance states that “trainees do not need to design, lead, and project manage entire QI projects to satisfy curriculum requirements”.
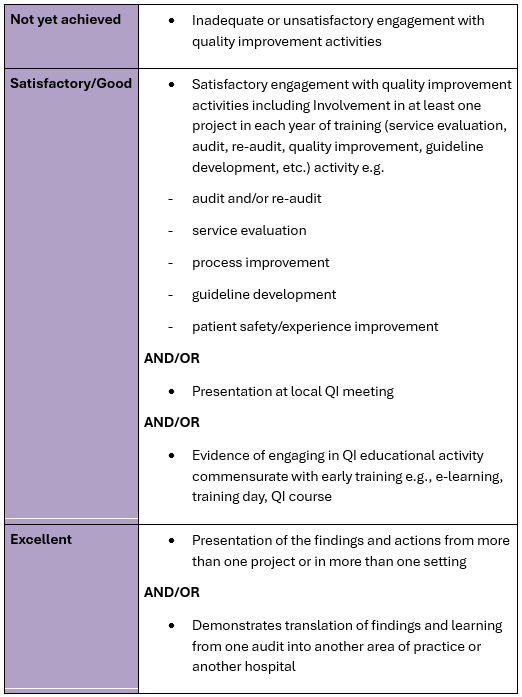
Standard required
The following table summarises the activity that is expected and how excellence might be pursued:
End of ACCS:
Educational review
Summative assessment each year is a judgement by the Educational Supervisor and recorded on the Intermediate ESR form, with subsequent overview from the ARCP panel. By the end of intermediate training, trainees are required to provide sufficient evidence to at least a satisfactory standard for the key capability of this SLO.
Review of the EM-QIAT
The Educational Supervisor gives a final rating following review of the EM-QIAT. This is reviewed along with all other SLOs at ARCP. Review of the EM-QIAT by the Educational Supervisors can be supported by appropriately trained departmental QI leads or other local equivalents.
Note that the Academy of Medical Royal Colleges in ARCP guidance states that “trainees do not need to design, lead, and project manage entire QI projects to satisfy curriculum requirements”
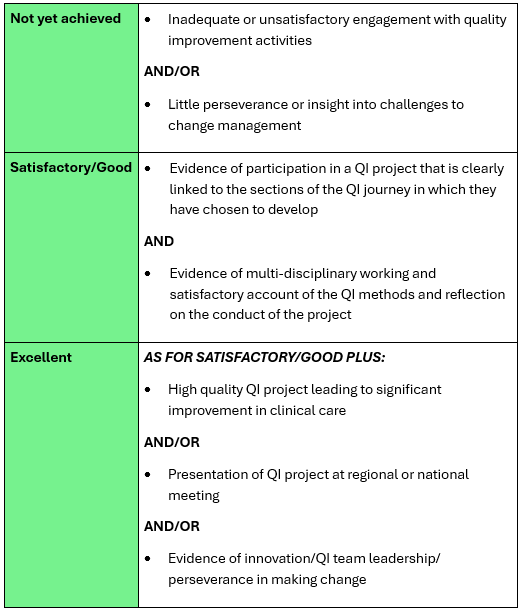
Standard required
The following table summarises the activity that is expected and how excellence might be pursued:
End of Intermediate
Educational review
Summative assessment each year is a judgement by the Educational Supervisor and recorded on the Higher ESR form, with subsequent overview from the ARCP panel. By the end of the three years of higher training, trainees are required to provide sufficient evidence to at least a satisfactory standard for the two key capabilities of this SLO.
Review of the EM-QIAT
The Educational Supervisor gives a final rating following review of the EM-QIAT. This is reviewed along with all other SLOs at ARCP. Review of the EM-QIAT by the Educational Supervisors can be supported by appropriately trained departmental QI leads or other local equivalents.
Note that the Academy of Medical Royal Colleges in ARCP guidance states that “trainees do not need to design, lead, and project manage entire QI projects to satisfy curriculum requirements”.
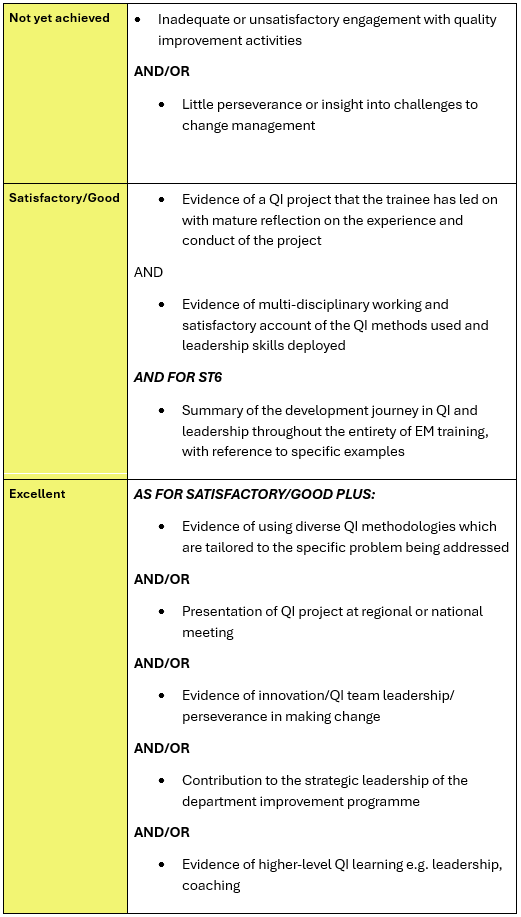
Standard required
The following table summarises the activity that is expected and how excellence might be pursued:
End of higher:
Creating Conditions
Start with ‘Why’ – TED talk Simon Sinek
Problem Identification
NHS Patient Safety Investigations
Patient & Public Involvement
Patient Public Involvement – King’s Improvement Science
Understanding Systems
Using systems thinking to identify the right problem
Developing Aims
Testing Changes
NHS England Innovation Accelerator
Friends & Family Test – NHS England
Methods for evaluation of small scale QI projects
Implementation
Evaluation: what to consider – the Health Foundation
Spread
NICE – writing the clinical guideline
Measurement
Quality Improvement: Choosing Measures
Understanding Variation in processes
A guide to creating and interpreting run and control charts
An introduction to analysing QI and QA data
How to guide for measurement for Improvement
Project Management & Communication
Project Management & Communication
How to Increase your Influence at Work
Leadership & Teams
EMLeaders:
Access to online modules – open to all 4 nations
10 principle of Good Interdisciplinary team-work
Overview & Combined Toolkits
Trainees Improving Patient Safety through Quality Improvement (TIPSQI)
Health Foundation – Quality improvement made simple – What everyone should know about Healthcare QI
Kotter’s Eight Steps of Change
AHSN North East & North Cumbria – Improvement toolkit
IHI Improvement Essential Toolkit
Online QI Training Courses
Each board/trust is highly likely to have their own version, please make enquiries locally. This is a selection of open access e-learning materials:
Scotland – all with TURAS login
Organisations
Healthcare Safety Investigation Branch
Institute for Healthcare Improvement (IHI)
Life QI – subscription platform – check with your organisation

